


Electronic Health Records (EHR) should lighten the load on clinicians, give leaders real‑time insight, and use public funds wisely. South Africa’s 2019 National Digital Health Strategy wants exactly that. Yet on the ward, nurses still juggle paper files and creaky software. Why?
The new study lays bare the daily headaches, especially with the long‑running Clinicom hospital system. This analysis unpacks those findings and shows how HealthOrbit AI’s MedOrbit—an Ambient AI Scribe—solves them.
The Current Landscape: Many Systems, Little Joy
Clinicom’s High Coverage but Low Clinician Happiness
Western Cape hospitals rolled out Clinicom two decades ago. Participants in the study called it “largely administrative with little clinical data” and admitted that clinicians rarely use it during consultations. Notes still start on paper, then clerks type them in later—double work that breeds errors and delays.
- 54 of 55 Western Cape hospitals run Clinicom, yet real‑time clinical entry remains rare.
- 2 of 37 Gauteng hospitals use any EHR at all—highlighting national fragmentation.
Common Grievances Heard in Interviews
| Pain Point | How It Shows Up in Clinicom Today |
| “Not really an electronic health record… more a patient inventory and accounting system.” | Clinicians flick between paper charts and screens, then re‑enter data. |
| “You need to demonstrate benefits; right now they feel like data capturers.” | Doctors spend extra minutes per patient just completing fields unrelated to care. |
| Limited clinical decision support | No prompts for drug interactions or guideline reminders. |
| Connectivity dips stall work | Data entry freezes; staff revert to notebooks, losing time and accuracy. |
Beyond Clinicom: Other Systems, Same Story
Tier.net, PHCIS, and DHIS each capture slices of information but rarely speak to one another. The study found nearly 40 % of public facilities lack reliable internet, making real‑time exchange impossible.
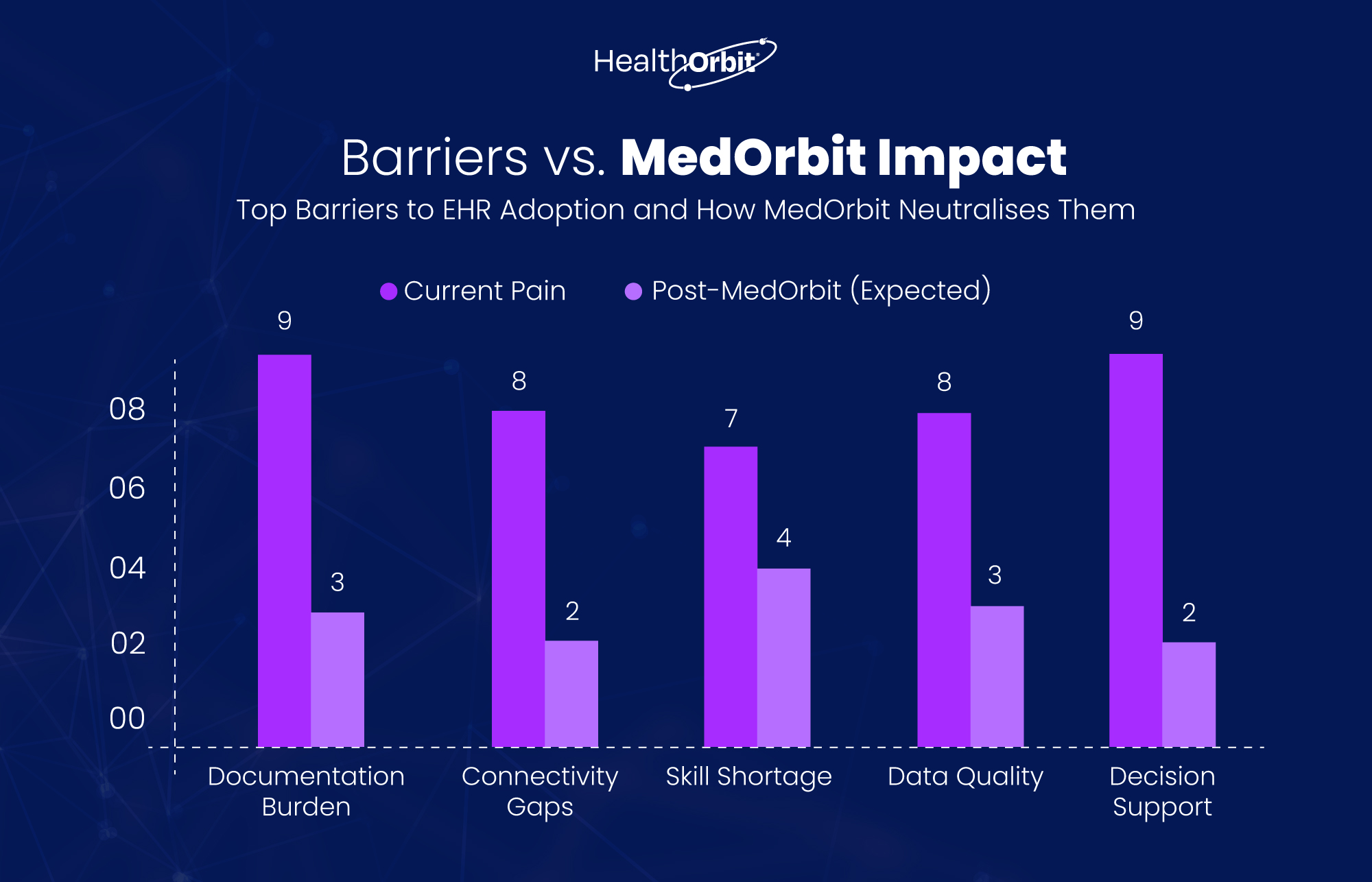
Four Structural Barriers Blocking Progress
- Leadership Instability – Frequent reshuffles and politically driven appointments stall long‑term tech planning.
- Skill Shortages – Government struggles to hire and keep IT talent; private sector rates outpace salaries.
- Weak Infrastructure – Almost 40 % of clinics go offline regularly; hardware sits boxed for months.
- Tender Troubles & Trust – Procurement favours connections, not capability; vendors grow wary.
The result? Static, siloed systems like Clinicom stay in place because ripping them out feels riskier than tolerating daily frustration.
Meet MedOrbit: The Ambient AI Scribe Built for South Africa’s Reality
| MedOrbit Feature | Why It Beats Clinicom |
| Voice‑first capture – records consults, turns speech into structured notes in seconds | Eliminates double data entry and paper reliance. |
| Multilingual support (65+ languages) with real‑time translation | Helps clinicians serve diverse patients; Clinicom stores English‑only fields. |
| Clinical Intelligence Co‑pilot – prompts on drug interactions, missing vitals | Adds decision support Clinicom lacks. |
| Offline‑first sync – captures data without internet, auto‑syncs later | Critical for facilities with 1 Mbps or less connectivity. |
| 30‑second document turnaround (SOAP note, referral letter, care plan) | Saves up to 70 % documentation time cited in global scribe studies. |
| Seamless EHR Integration – HL7/FHIR APIs slot into legacy systems | Modernises Clinicom rather than replacing overnight. |
| Regulatory Ready – HIPAA, GDPR, ISO 27001, DCB0129, DSPT, Cyber Essentials | Meets compliance headaches clinicians raise in audits. |
What the Study Says—and How MedOrbit Answers
“They are capturing on paper and handing to a clerk to type. That is not an EHR where the clinician can use it during consultation.”
Fix: MedOrbit transcribes the consult live, generates structured notes instantly, and surfaces them on‑screen for real‑time use.
“Our biggest challenge is the human factor… breaches happen when data are shared accidentally.”
Fix: MedOrbit enforces role‑based access, logs every action, and encrypts recordings—reducing accidental leaks.
“Nearly 40 % of facilities have no reliable internet.”
Fix: Offline capture ensures no lost notes; syncs when 3G returns.
“Clinicians feel they’re above typing—they must see benefits.”
Fix: Voice‑first design slashes typing to near‑zero; AI Co‑pilot returns helpful suggestions, showing immediate value.
A Phased Roadmap Using MedOrbit
- Pilot in Internet‑Ready Metros – Demonstrate 70 % time savings; build clinician champions.
- Layer on Offline Clinics – Deploy mobile units; sync nightly.
- Integrate with Clinicom & Tier.net – Use FHIR bridges for incremental data sharing.
- Scale Nationally with NHI Roll‑out – Align with Health Normative Standards Framework; unify patient IDs.
- Continuous Training & Feedback – In‑app tips plus on‑site super users.
Conclusion: Stop Muddling Through, Start Moving Forward
South Africa’s clinicians deserve an EHR that works during the consult, not hours later. Clinicom’s administrative skeleton served its era, but now slows care, frustrates staff, and fragments data. The study confirms these pain points loud and clear.
HealthOrbit’s MedOrbit Ambient AI Scribe meets South Africa, where it is: offline‑prone, multilingual, short on admin staff, and hungry for clinical decision support. It strips paperwork, lifts data quality, and plugs smoothly into existing systems—without another decade‑long overhaul.
Ready to see it live? Book a HealthOrbit AI’s MedOrbit demo or try it free and watch documentation times drop before your next tea break.





